19 Muscular tissue
Muscle tissue is characterised by properties that allow movement. Muscle cells are excitable; they respond to a stimulus. They are contractile, meaning they can shorten and generate a pulling force. When attached between two movable objects, in other words, bones, contractions of the muscles cause the bones to move. Some muscle movement is voluntary, which means it is under conscious control. Other movements are involuntary, meaning they are not under conscious control.
 Example
Example
Voluntary muscle contraction – a filly choosing to trot across the pasture to meet you, or a cow deciding to swish its tail to shoo away flies.
Involuntary muscle contraction – the contraction of pupils in bright light, beating of a heart, or digestion of food.
Classification of muscle tissues
Muscle tissue is classified into three types according to structure and function: skeletal, cardiac, and smooth (Table 4.1).
Table 4.1 Comparison of structure and properties of muscle tissue types
| Tissue | Histology | Function | Location |
| Skeletal | Long cylindrical fibre, striated, many peripherally located nuclei | Voluntary movement, produces heat, protects organs | Attached to bones and around entrance points to body (e.g., mouth, anus) |
| Cardiac | Short, branched, striated, single central nucleus | Contracts to pump blood | Heart |
| Smooth | Short, spindle-shaped, no evident striation, single nucleus in each fibre | Involuntary movement, moves food, involuntary control of respiration, moves secretions, regulates flow of blood in arteries by contraction | Walls of major organs and passage ways |
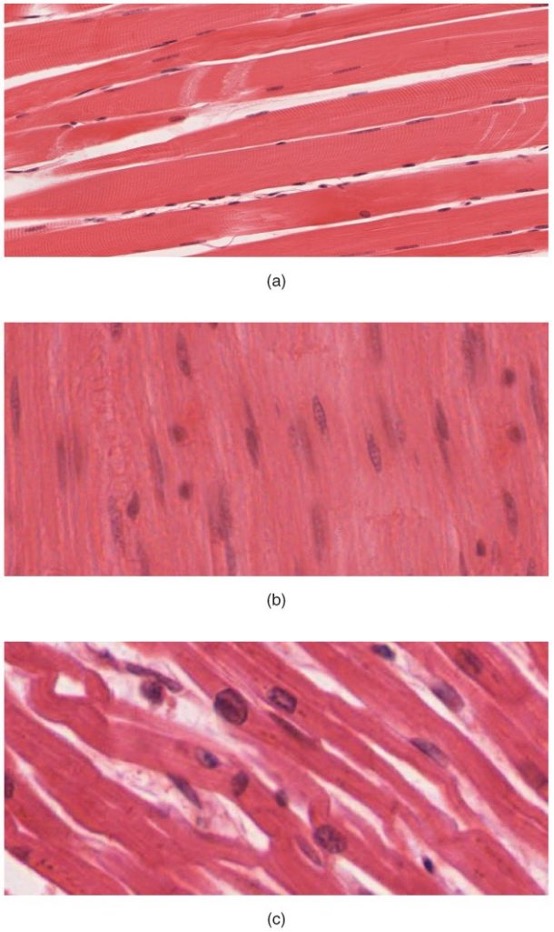
Skeletal muscle is attached to bones and its contraction makes possible locomotion, facial expressions, posture, and other voluntary movements of the body. Forty percent of your body mass is made up of skeletal muscle. Skeletal muscles generate heat as a by-product of their contraction and thus participate in thermal homeostasis. Shivering is an involuntary contraction of skeletal muscles in response to perceived lower than normal body temperature. The muscle cell, or myocyte, develops from myoblasts derived from the mesoderm. Myocytes and their numbers remain relatively constant throughout life. Skeletal muscle tissue is arranged in bundles surrounded by connective tissue. Under the light microscope, muscle cells appear striated with many nuclei squeezed along the membranes. The striation is due to the regular alternation of the contractile proteins, actin and myosin, along with the structural proteins that couple the contractile proteins to connective tissues. The cells are multinucleated as a result of the fusion of the many myoblasts that fuse to form each long muscle fibre.
Cardiac muscle forms the contractile walls of the heart. The cells of cardiac muscle, known as cardiomyocytes, also appear striated under the microscope. Unlike skeletal muscle fibres, cardiomyocytes are single cells typically with a single centrally located nucleus. A principal characteristic of cardiomyocytes is that they contract on their own intrinsic rhythms without any external stimulation. Cardiomyocyte attach to one another with specialised cell junctions called intercalated discs. Intercalated discs have both anchoring junctions and gap junctions. Attached cells form long, branching cardiac muscle fibres that are, essentially, a mechanical and electrochemical syncytium allowing the cells to synchronise their actions. The cardiac muscle pumps blood through the body and is under involuntary control. The attachment junctions hold adjacent cells together across the dynamic pressures changes of the cardiac cycle.
Smooth muscle tissue contraction is responsible for involuntary movements in the internal organs. It forms the contractile component of the digestive, urinary, and reproductive systems as well as the airways and arteries. Each cell is spindle shaped with a single nucleus and no visible striations (Figure 4.14).
 Reflective question
Reflective question
What type of muscle do you expect your tongue is? Is this a voluntary or involuntary muscle?

 Case study
Case study
A 4-year-old Yearling Colt presents with stiffness, muscle tremors, and reluctance to move after a training session. The owner reports that the horse has been sweating excessively and appears to be in pain. Upon physical examination, you note firm, painful muscles, particularly in the hindquarters. The horse shows signs of distress and discomfort.
Serum Creatine Kinase (CK) is elevated at 15,000 U/L (normal range: 100-300 U/L), indicating muscle damage.
Serum Aspartate Aminotransferase (AST) is also elevated, further supporting muscle injury.
Urinalysis shows dark-colored urine, positive for myoglobin, confirming muscle breakdown.
The diagnosis is exertional Rhabdomyolysis, also known as “tying-up” and involves muscle damage due to intense exercise. It is characterised by muscle pain, stiffness, and the release of muscle enzymes into the bloodstream.
Treatment includes rest to prevent further muscle damage and fluid therapy (intravenous fluids) to flush out myoglobin and prevent kidney damage.


{kind=link}